Modern digital hearing aids incorporate amazing electronic advancements over hearing technology because of computerization. The circuits are so miniaturized that they can fit into smaller devices and at the same time process sound with space-age efficiency. With millions and now billions of operations, these ear level computers can control feedback, loudness discomfort, and reduce noise, while maximizing word clarity. In fact, when advanced technology is correctly prescribed and verified for sound accuracy and brain training, most patients receive significant benefit. For those that hearing aids are not beneficial because of severe to profound deafness, Cochlear Implants are a modern miracle, “a real game changer”.
All premium hearing instruments are essentially the same devices with a variety of options for technology level, style, size, color, controls, automation, connectivity (FM, cable, and Bluetooth), and programmability. When set on the same prescriptions, benefits and fitting issue remain universal. For most, the outcome of buying hearing aids and services should include being able to hear a whisper or soft voice, having an ease of hearing in daily situations, feeling comfortable with the physical fit, and sound loudness, and improved hearing skills. For those with moderate or greater impairment, an adjustment that reduces background noise while selecting speech signals is recommended. However, modern technology cannot repair all patterns of nerve cell damage. Therefore, some degree of communication loss is to expected based on severity.
Marketing Breakthroughs
Although hearing aid marketing suggests that there is a wide variety of differences between products with “amazing breakthroughs.” Almost all of the features promoted in the media are available in some form or another from the top six manufacturers. The variety of devices available meet a wide range of needs.
In addition to conventional hearing aids, ear level personal amplifiers are being sold as low cost hearing devices, they are not hearing aids. These devices are for those who want to self-diagnose and fit themselves, like cheater glasses when just a little power is needed. These can be helpful for patients with mild hearing loss and for some approaching moderate loss. However, most self-fitted amplifiers will under perform as hearing becomes worse compromising brain function. At this point, hearing aids with properly selected sound processing and verified prescriptions are needed. Buyers should be prepared to return the devices if they have too much noise, sound discomfort, poor fit or soreness, or sound distortion and squealing. If it cannot be worn all day in comfort, it is not training the brain.
Hearing Aid Providers
Hearing aids have been around since the advent of the first ear trumpets sold in pharmacies in the late 1800’s. Modern advances in electronic hearing aids were not realized until the late 1980’s, although ear level amplifiers were manufactured by Zenith in the 1950’s. The digital age, in the mid 1990’s, changed the ability of hearing aids to control sound, noise, and feedback, and reduce the size, while improving comfort. Currently, tremendous changes in technology and Audiology services have altered the direction of hearing care. Programming hearing aids to change the brain’s sound map to promote learning or using remote control amplification for children with sound processing problems are a couple of examples of how complex this can be. A qualified Audiologist will select a manufacturer and product that matches the patient’s physical (dexterity – size and adjust ability) and psychological needs (dementia – transparent and automatic), correlate the prescription with the patient’s hearing needs using scientific methods, provide appropriate services and counseling for each patient, while insuring that brain activity is eventually maximized.
Audiologist have a masters or doctorate degree in Audiology or both, Board Certification in Audiology (ABA) or a Certificate of Clinical Competence in Audiology (CCC-A), years of experience, and provide more services than just hearing aids. These added services include diagnostic testing and treatments for tinnitus, hyperacusis, and central auditory processing disorders. This is because these are directly related to the fitting of hearing aids and patient counseling and success. In addition to Audiologists, Hearing Aid Dispensers fit hearing aids, and ENT physicians may have a hearing aid dispensary.
Evaluation, Options, and Outcome
The following Audiological services, hearing aid options, and protocols are recommended as part of the hearing aid and hearing training/learning process. These services along with motivation and readiness to wear hearing aids will ensure success. Very few patients should fail to get benefit from hearing aids or cochlear implants.
1.Hearing Assessment
The purpose of this assessment is to obtain sufficient diagnostic information to determine the cause, type, location, and level of the hearing loss and associated processing disorders. Furthermore, the results will determine the candidacy for amplification, identify medical conditions requiring an ENT specialist or Neurologist, and provide direction for counseling patients and family members. For those with auditory processing disorders, the assessment will also include a battery of additional specialized tests.
2.Needs Assessment
The purpose of this assessment is to consideration the factors necessary to meet the patient’s hearing needs at home, work, school, or play. This includes a discussion on the benefits, limitations, and costs associated with obtaining amplification and other devices.
3. Selection and Special Features
The selection of hearing aids should be based on the degree of hearing loss, power needed to meet the prescription, the shape and size of the ear, jaw movement, wax development, and the patient’s ability to operate the devices. In general, hearing loss greater than mild to moderate are best fit with advanced technology because of benefits to reduce feedback, and improve fidelity and noise reduction. Furthermore, special features, such as connectivity devices for television and telephone and other devices are available for most devices. When properly selected, the features listed below (A-J) can greatly enhance hearing.
A. Do I need a digital hearing aid?
The entire industry has moved all hearing aids to digital computer status. Older analogue technology is phased-out and only available in over the counter self-fitting personal amplifiers.
B. Do I need feedback cancellation?
There are a number of feedback controllers (feedback is a squealing sound) available in advanced technology that can essentially eliminate this annoyance. Feedback control has been lacking over the years requiring a lowering of needed power to the ear. Presently, newer devices can control feedback, in most cases, and at the same time give a wider range of sound power resulting in better understanding. Feedback control is especially important if there is a small ear canal, an open ear fitting, or in cases of severe to profound hearing loss, extreme power.
C. Do I need directional microphones?
One of the most remarkable changes in hearing aid technology is in the area of noise reduction. The combination of digital noise cleaning and directional or speech processing microphones allow the instruments to clean the speech and noise signals and share the information between the ears to coordinating the locations of sound and speech. This is more effective for mild to moderately severe degrees of hearing loss, but still useful for those with all levels of loss and is universally recommended where available.
D. Do I need a t-coil?
The use of t-coil friendly systems is expanding in the United States (T-Coils News). A t-coil is a magnetic device that picks up sound directly from another magnetic signal such as that from an earpiece of the telephone, a classroom sound system (room wire floor loop), or a neck loop connected to broadcasts from Bluetooth or FM audio devices. If it makes sound, the t-coil can be used to attach hearing aids to the world. This product is highly recommended by the Hearing Loss Association of America (HLAA) and professionals in Deaf Education, Otolaryngology, and Audiology. For public areas, the American Academy of Audiology and HLAA have joined together to promote the Loop America initiative to help groups with understanding and implementing the technology (http://www.hearingloop.org/).
E. Do I need direct audio input (DAI) connections?
In severe to profound hearing loss, for patients using behind-the-ear (BTE) hearing aids, a special connection can be used to input sound signals from a variety of devices. Some devices do not have FM or Bluetooth connectivity and a direct connection is needed such as an industrial radio system. This is accomplished by using a boot or plug that connects to the hearing aid or when desired a Cochlear Implant.
F.Do I need two hearing aids?
If you have hearing loss in both ears binaural hearing aids are a necessity. Hearing is a learned function that needs maintenance. The purpose of using two hearing aids is to map and continually remap the brain for the best possible information sharing. The ears work together to enhance the understanding of speech, locate sound, and decrease noise interference. There are two exceptions, these are seniors with an unusable or dead ear and those with some forms of auditory processing disorders. For single sided deafness, a single hearing aid or receiver should be immediately used on the good ear with a Cros or BiCros wirelessly connected mic transmitter on the poorer ear.
G.Does the size of the hearing aid matter?
Our fondest dream is to use the smallest hearing aids that are practically invisible, last forever, and have superior performance. Unfortunately, the smallest hearing aids can service not all ears and degrees of hearing loss nor do they last forever or are always amazing. The smallest hearing aids are called completely in-the-canal (CIC) and can be an excellent device when fitted to the right patient, usually mild to moderate hearing loss, limited wax, a clear path into the canal, and the dexterity to use it. However, CIC hearing aids or Lyric (Disposable Deep Canal) are not recommended for severe to profound hearing loss or for small ears, those with Auditory Processing Disorders, or those that develop considerable wax. CIC hearing aids have the most repairs and the Lyric has to be replaced every three months. In all cases, the size and shape of the hearing aids must match the physical fit and use, needed options (microphones, battery, and memory button) and the power requirements. The CIC fittings represent less than 8% of all hearing aid users.
Even a smaller group are using the deep canal amplifier, Lyric, the most expensive hearing devices on the market. They are replaced, back near the eardrum, every three months. There are few patients that wear it, but for those that it is successful, it can be very nice to hear 24/7. A backup set of conventional hearing aids is always recommended because of failure or physical discomfort.
H.Do I need an open mold hearing aid fitting?
For hearing losses that have normal hearing in the low tones and only high tone hearing loss as seen in the audiogram, an open fitting is a must. If hearing ability in the low pitches (the pitch range one hears when saying “eeee” and “rrrrr”) is near normal, then an open mold fitting is needed. This “eeee” to “rrrrrr” range in a man’s voice is a low tone sound (100 Hz) and women are higher (200 Hz). When this range is normal, filling the ears with hearing aids will close off the head’s normal low tone exit, the ear canal. When occluded, the result is a clogged sensation in the head, something like a cold making the voice sound hollow, muffled, or reverberating in the head. This is called occlusion. The only way to relieve this pressure is to use an open mold fitting of special earmolds that are non-occluding or open.
I.Do I need wireless communication and coordination between my hearing aids?
This feature is found in a variety of hearing aids and can be very helpful in adjusting programs for noise reduction, volume, and microphone features. The technology also couples both hearing aids so that the user can make a change in function by pushing the button on one side that changes the function in both. Additionally, the use of remote controls or cell phones communication can be used to adjust the hearing aids, control a remote microphone or t-coil, and hear on a Bluetooth cell phone.
J.Do I need additional connectivity devices to augment the use of my hearing aids?
Some hearing impaired listeners can use products to improve hearing on the telephone and television, computer or monitor, and in the near future turn on home appliances on activation of the battery. Specialty products can connect both cochlear implants and hearing aids together to connect to TV and telephones. Some products have battery rechargers that require no physical work; just pop the whole hearing aid into the charger.
4.Verification
This stage of the hearing aid fitting process is more important than the choice of hearing aid manufacturer. This is because, it is the verification that conforms the hearing aid to the individual and their hearing loss. Verification starts with an evaluation of physical fit and comfort to insure that the hearing aid is secure, but not too tight to cause pressure or discomfort in the ear canal. Following physical fit, the purpose of verification is to guarantee that the hearing aid prescription actually fits the hearing loss. Computer automated fittings provided by the manufacturers without real ear testing is substandard care and may limit the potential benefit. Verification is done by performing a remarkable set of tests called real ear probe or speech mapping. During these procedures, a tiny microphone tube is inserted into the ear canal along with the hearing aid. When the hearing aid amplifies sound, it can be measured and adjusted via computer to maximize power and performance. The attached figure shows that the manufacturer’s prescription in black, which should mirror the top red lines does not fit the hearing loss. This error exists in over 60% of hearing aid sold. After this verification is performed, it will be necessary for the final changes to the prescription to be customized by the Audiologist.
For very young children, this testing is done using a protocol called real ear to coupler difference (RECD). This testing is used to determine fitting accuracy in place of real ear tests that require patient cooperation. Children require a completely different set of services related to development and speech and language, amongst others (The Early Years).
5. Orientation and Counseling
After the physical and acoustic fit of the hearing aids have been accomplished, this is followed by training on the insertion and removal of the instruments, changing batteries, turning the device on and off, operating the different sound programs, and learning how to use the telephone and other compatible devices. Maintenance of the hearing aids, including cleaning and removal of wax and moisture is also reviewed. Listening skills instruction that help patients to function in common hearing situations are also typically provided during the initial adjustment period. In some cases, auditory training and hearing neuroplasticity therapy will be recommended to improve hearing performance.
6. Adaptation
During this final training, the information from the ears is used to map the cortex and hearing networks. This activity, over time, trains the brain to function better as a result of sound exposure and experience, just like infants. The typical time it initially takes to adapt to hearing aids is between 30 and 60 days for adults, but it is not until three months or more before the brain has enough experience to reprogram sound into memory and start the building of a complete library. That library needs maintenance and daily use. For very young children this process is occurs along with a maturing hearing system and new sounds are integrated as part of the development, fostering speech and language. For seniors, it may take longer as aging may play a role in reducing performance and learning, but ultimately patients are successful.
7. Validation
The most important aspect of hearing aid use is how well they work in a variety of situations. One way to accomplish this is to compare the aided results with the initial hearing questionnaire taken prior to using hearing aids. Another way to measure performance is to determine the improvements based on a set of individual goals such as, hearing better at home or group meetings. Based on the realistic expectations provided by the Audiologist, the results of hearing performance should demonstrate considerable improvement hearing in quiet surroundingsand good to excellent performance in comfort and understanding in background noise for most patients depending upon the degree of nerve damage. For some, hearing aids will be able to reduce noise, but will also not provide enough clarity, regardless of the manufacturer.
Hearing Performance and Brain Maintenance
The purpose of using hearing aids and other devices is to improve quality of life by preserving engagement through ease of hearing, while reducing isolation or irritation. When hearing aids are fitted correctly and the services are more than just a sale by a technician, patients should have maximum hearing aid performance with a measured outcome. All patients should recognize that hearing aids are of great importance in their daily lives and without them there is a lack of interaction. The research literature is clear, making hearing loss one of the higher risk maladies for memory loss, dementia, and even Alzheimer’s disease (Central Presbycusis).

 instruments are essentially the same devices with a variety of options for technology level, style, size, color, controls, automation, connectivity (FM, cable, and Bluetooth), and programmability. When set on the same prescriptions, benefits and fitting issue remain universal. For most, the outcome of buying hearing aids and services should include being able to hear a whisper or soft voice, having an ease of hearing in daily situations, feeling comfortable with the physical fit, and sound loudness, and improved hearing skills. For those with moderate or greater impairment, an adjustment that reduces background noise while selecting speech signals is recommended. However, modern technology cannot repair all patterns of nerve cell damage. Therefore, some degree of communication loss is to expected based on severity.
instruments are essentially the same devices with a variety of options for technology level, style, size, color, controls, automation, connectivity (FM, cable, and Bluetooth), and programmability. When set on the same prescriptions, benefits and fitting issue remain universal. For most, the outcome of buying hearing aids and services should include being able to hear a whisper or soft voice, having an ease of hearing in daily situations, feeling comfortable with the physical fit, and sound loudness, and improved hearing skills. For those with moderate or greater impairment, an adjustment that reduces background noise while selecting speech signals is recommended. However, modern technology cannot repair all patterns of nerve cell damage. Therefore, some degree of communication loss is to expected based on severity. pharmacies in the late 1800’s. Modern advances in electronic hearing aids were not realized until the late 1980’s, although ear level amplifiers were manufactured by Zenith in the 1950’s. The digital age, in the mid 1990’s, changed the ability of hearing aids to control sound, noise, and feedback, and reduce the size, while improving comfort. Currently, tremendous changes in technology and Audiology services have altered the direction of hearing care. Programming hearing aids to change the brain’s sound map to promote learning or using remote control amplification for children with sound processing problems are a couple of examples of how complex this can be. A qualified Audiologist will select a manufacturer and product that matches the patient’s physical (dexterity – size and adjust ability) and psychological needs (dementia – transparent and automatic), correlate the prescription with the patient’s hearing needs using scientific methods, provide appropriate services and counseling for each patient, while insuring that brain activity is eventually maximized.
pharmacies in the late 1800’s. Modern advances in electronic hearing aids were not realized until the late 1980’s, although ear level amplifiers were manufactured by Zenith in the 1950’s. The digital age, in the mid 1990’s, changed the ability of hearing aids to control sound, noise, and feedback, and reduce the size, while improving comfort. Currently, tremendous changes in technology and Audiology services have altered the direction of hearing care. Programming hearing aids to change the brain’s sound map to promote learning or using remote control amplification for children with sound processing problems are a couple of examples of how complex this can be. A qualified Audiologist will select a manufacturer and product that matches the patient’s physical (dexterity – size and adjust ability) and psychological needs (dementia – transparent and automatic), correlate the prescription with the patient’s hearing needs using scientific methods, provide appropriate services and counseling for each patient, while insuring that brain activity is eventually maximized. The entire industry has moved all hearing aids to digital computer status. Older analogue technology is phased-out and only available in over the counter self-fitting personal amplifiers.
The entire industry has moved all hearing aids to digital computer status. Older analogue technology is phased-out and only available in over the counter self-fitting personal amplifiers. One of the most remarkable changes in hearing aid technology is in the area of noise reduction. The combination of digital noise cleaning and directional or speech processing microphones allow the instruments to clean the speech and noise signals and share the information between the ears to coordinating the locations of sound and speech. This is more effective for mild to moderately severe degrees of hearing loss, but still useful for those with all levels of loss and is universally recommended where available.
One of the most remarkable changes in hearing aid technology is in the area of noise reduction. The combination of digital noise cleaning and directional or speech processing microphones allow the instruments to clean the speech and noise signals and share the information between the ears to coordinating the locations of sound and speech. This is more effective for mild to moderately severe degrees of hearing loss, but still useful for those with all levels of loss and is universally recommended where available. audio devices. If it makes sound, the t-coil can be used to attach hearing aids to the world. This product is highly recommended by the Hearing Loss Association of America (HLAA) and professionals in Deaf Education, Otolaryngology, and Audiology. For public areas, the American Academy of Audiology and HLAA have joined together to promote the Loop America initiative to help groups with understanding and implementing the technology (http://www.hearingloop.org/).
audio devices. If it makes sound, the t-coil can be used to attach hearing aids to the world. This product is highly recommended by the Hearing Loss Association of America (HLAA) and professionals in Deaf Education, Otolaryngology, and Audiology. For public areas, the American Academy of Audiology and HLAA have joined together to promote the Loop America initiative to help groups with understanding and implementing the technology (http://www.hearingloop.org/).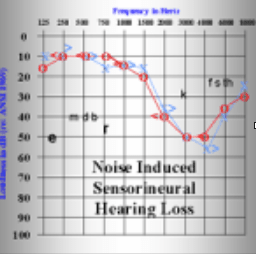 hearing loss as seen in the audiogram, an open fitting is a must. If hearing ability in the low pitches (the pitch range one hears when saying “eeee” and “rrrrr”) is near normal, then an open mold fitting is needed. This “eeee” to “rrrrrr” range in a man’s voice is a low tone sound (100 Hz) and women are higher (200 Hz). When this range is normal, filling the ears with hearing aids will close off the head’s normal low tone exit, the ear canal. When occluded, the result is a clogged sensation in the head, something like a cold making the voice sound hollow, muffled, or reverberating in the head. This is called occlusion. The only way to relieve this pressure is to use an open mold fitting of special earmolds that are non-occluding or open.
hearing loss as seen in the audiogram, an open fitting is a must. If hearing ability in the low pitches (the pitch range one hears when saying “eeee” and “rrrrr”) is near normal, then an open mold fitting is needed. This “eeee” to “rrrrrr” range in a man’s voice is a low tone sound (100 Hz) and women are higher (200 Hz). When this range is normal, filling the ears with hearing aids will close off the head’s normal low tone exit, the ear canal. When occluded, the result is a clogged sensation in the head, something like a cold making the voice sound hollow, muffled, or reverberating in the head. This is called occlusion. The only way to relieve this pressure is to use an open mold fitting of special earmolds that are non-occluding or open.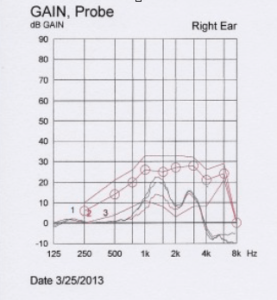 and television, computer or monitor, and in the near future turn on home appliances on activation of the battery. Specialty products can connect both cochlear implants and hearing aids together to connect to TV and telephones. Some products have battery rechargers that require no physical work; just pop the whole hearing aid into the charger.
and television, computer or monitor, and in the near future turn on home appliances on activation of the battery. Specialty products can connect both cochlear implants and hearing aids together to connect to TV and telephones. Some products have battery rechargers that require no physical work; just pop the whole hearing aid into the charger. hearing questionnaire taken prior to using hearing aids. Another way to measure performance is to determine the improvements based on a set of individual goals such as, hearing better at home or group meetings. Based on the realistic expectations provided by the Audiologist, the results of hearing performance should demonstrate considerable improvement hearing in quiet surroundings and good to excellent performance in comfort and understanding in background noise for most patients depending upon the degree of nerve damage. For some, hearing aids will be able to reduce noise, but will also not provide enough clarity, regardless of the manufacturer.
hearing questionnaire taken prior to using hearing aids. Another way to measure performance is to determine the improvements based on a set of individual goals such as, hearing better at home or group meetings. Based on the realistic expectations provided by the Audiologist, the results of hearing performance should demonstrate considerable improvement hearing in quiet surroundings and good to excellent performance in comfort and understanding in background noise for most patients depending upon the degree of nerve damage. For some, hearing aids will be able to reduce noise, but will also not provide enough clarity, regardless of the manufacturer.